

![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
 .
.
Journal of Clinical Endocrinology 1958; 18:1102-1110.
EFFECT OF FLUORINE ON THYROIDAL IODINE METABOLISM IN HYPERTHYROIDISM
PIERRE-M. GALLETTI, M.D., PH.D* AND GUSTAVE JOYET, D.Sc.
The Department of Medicine and Radiology, Kantonspital, Zurich, Switzerland
ABSTRACT: Prolonged administration of a daily dose of 5-10 mg. of fluoride to patients with hyperthyroidism may cause clinical improvement together with a significant fall in the level of plasma protein-bound iodine and a reduction in the basal metabolic rate. Studies with radioactive fluorine failed to demonstrate any important accumulation of fluorine within the thyroid in vivo. Thyroidal, blood and urinary radioiodine studies suggest that fluorine inhibits the thyroid iodide-concentrating mechanism. Fluorine does not impair the capacity of the gland to synthesize thyroid hormone when there is an abundance of iodide in the blood. However, inhibition of the thyroidal concentrating capacity when the total iodide pool is low will impose a critical limitation of hormonal synthesis, and may explain the therapeutic effect.
THE widespread use of fluoride to reduce dental caries has aroused considerable controversy because of the toxicity of this halogen. Under the conditions of relative iodine deficiency of Central Europe, a possible thyroid-inhibiting action of fluorine has elicited the interest of physicians and public health officers. Previous studies on animals and human beings did not demonstrate any significant and reproducible alterations of thyroidal function due to small doses of fluorine which did not exceed a daily intake of 2.0 mg (approximately the doses used for prophylaxis of dental caries). In, man, however, administration of larger doses over a longer period of time caused a noticeable reduction of several parameters of thyroidal biologic activity (1-5).
Several authors postulated that goitrous states may be attributed to fluorine intake and, conversely, that this element can be utilized in the treatment of hyperthyroidism (6-8). Other investigators, however, could not reproduce these definite changes in the thyroid, and thus the thyreostatic activity of fluorine is still questioned. Since the hyperfunctioning thyroid is a more sensitive structure than the normal gland, we studied the effect of fluorine on patients with hyperthyroidism. Few clinical studies are concerned with physiologic and toxic effects of fluorine over long periods (9). Therefore this investigation was limited to intelligent and reliable patients in whom the course of the disease as well as the intake of prescribed doses and the possible appearance of toxic manifestations could be carefully controlled.
METHODS
Fluorine (in the form of sodium fluoride) was given, orally for the most part, three times daily. Patients who received it intravenously were given a single injection daily. The doses recorded here express the quantity of fluorine (F)- in ionized form. Despite the relatively large amounts administered (up to 20 mg. of F- for one injection), neither immediate nor delayed toxic manifestations were observed. Patients with severe hyperthyroidism who were not sufficiently improved after fluorine therapy could not be observed for more than six weeks.
In 15 patients, the basal metabolic rate (BMR) and the level of plasma protein-bound iodine (PBI) were determined before and after the administration of 2-10 mg. of F- over a period ranging from 20 to 245 days. In 10 patients, the action of fluorine was checked by repeated radioiodine tests (10). The initial slope (To') of the uptake curve, which equals the uptake rate of the inorganic iodine of the plasma by the thyroid (11, 12), was taken as an indicator of the cumulative, but usually weak inhibiting action of fluorine.
In 4 cases, simultaneous intravenous injections of 20 mg. of F- and 10-50 uc. of carrier-free I131 were given one week after a previous dose of I131 alone, to test the possibility of a mass-action effect due to a high level of plasma fluorine. Thyroidal concentration and urinary excretion of radioactive fluorine were studied in 2 cases. F18 was obtained by irradiating an aqueous solution of NaF (20 mg. of F-), as described elsewhere (5).
RESULTS
BMR and PB1
In 6 of the 15 patients studied, the symptoms of hyperthyroidism were relieved and both the BMR and the plasma PBI concentration fell to normal levels. In 9 other cases, fluorine was clinically ineffective, although an improvement in the BMR or PBI level was often observed. The drop of the mean value for plasma PBI from 9.8 to 6.7,ug. per 100 ml. and of the mean value for the BMR from +37 to +27 per cent indicated definite inhibition of thyroid hyperfunction. In 9 patients the fall of the PBI level was significantly greater than twice the standard deviation of an isolated determination as checked by duplicate measurements. The BMR decreased significantly in 7 cases.
I131 tests
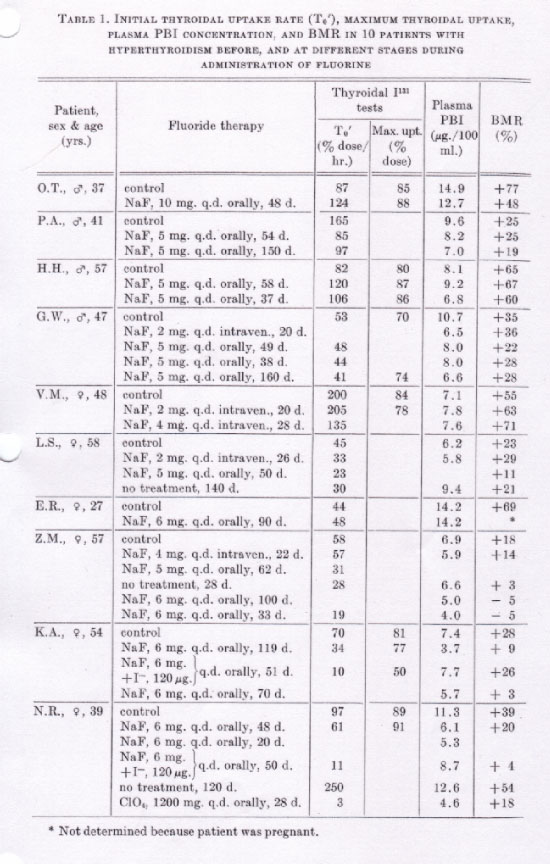
Repeated radioiodine tests on 6 female and 4 male patients (Table 1) showed the following:
{kind=link}
1) An inhibitory effect of fluorine on the initial thyroidal I131 uptake was noted in 7 of 10 patients. In 4 of them (Z. M., L. S., K. A. and N. R.) the value of To' was reduced to the normal range (Fig. 1) by administration of fluorine over a period of 67 to 245 days. Though not as sensitive a test as the I131 uptake rate, the maximum uptake decreased, and thyroidal activity during the first week was also modified (Fig. 2).
2) A definite effect of fluorine usually appeared only after 40-50 days. In 3 patients with moderate or severe hyperthyroidism (P. A., G. W. and V. M.) inhibition of the thyroidal uptake of inorganic iodine resulted in no significant improvement of the clinical picture, and therapy was considered ineffective.
3) In 2 patients (L. S. and N. R.) who showed clinical improvement with a corresponding fall of To' to the normal level, interruption of fluorine intake was followed by a relapse of the hyperthyroidism, associated with a rise in the initial slope of the thyroidal iodine uptake.
4) In 2 patients (K. A. and N. R.) with moderate thyroid hyperfunction in whom To' was evidently lowered by fluoride therapy, a minimum dosage of inorganic iodine (100-120 ug. of I- daily) was added to the fluorine intake. Patient K. A. (recurrence of hyperthyroidism after subtotal thyroidectomy) was clinically cured by fluorine therapy over a period of four months, though a small nodular goiter developed. Administration of iodine caused such a spectacular relapse that it had to be stopped after six weeks. The goiter, which during iodine therapy was no longer palpable, reappeared when hyperthyroidism was controlled by means of fluorine alone. In Patient N. R., the addition of iodine did not alter the clinical effect of fluorine therapy to the same extent. However, there was a recurrence of palpitation. As soon as the PBI level rose, therefore, the administration of iodine was discontinued. The patient progressed satisfactorily with fluorine alone for about two months; then she escaped our observation. When seen four months later, she again presented the signs of severe hyperthyroidism. Treatment with sodium perchlorate quickly brought the disease under control.
I131-NaF tests
No inhibition of the rate of thyroidal iodine uptake was observed when fluoride was injected in excess simultaneously with carrier-free radioiodine. On the contrary, the sharp rise of the plasma fluoride level resulted in a slight increase of the thyroidal uptake rate of inorganic iodine in the 4 cases tested.
F18 tests
Radiofluorine was injected into a subject with a normal thyroidal iodine uptake and into a patient with severe hyperthyroidism. In both cases comparison of the radioactivity in the region of the thyroid with that in the region of the precordium did not show any appreciable thyroidal uptake (i.e., less than 1 per cent per hour) of F18, irrespective of the uptake rate of iodine. The rate of urinary excretion of fluorine (29 and 49 per cent per hour) was in the upper range of the urinary excretion rate for iodine.
Clinical observations
The signs and symptoms of hyperthyroidism were completely relieved by administration of fluorine in 6 of 15 patients; tachycardia and tremor disappeared within four to eight weeks and loss of weight was stopped. The greatest clinical improvement was observed in women between 40 and 60 years of age with a moderate degree of thyrotoxicosis. Young patients with the classic picture of Graves' disease did not respond at all to fluorine therapy. In all cases but 1, enlargement of the thyroid was inconspicuous. In a case of severe hyperthyroidism associated with bilateral exophthalmos, congestion of the eyeballs and chemosis were not benefited by fluorine therapy; the proptosis, however, regressed. No other metabolic effects of fluorine were observed.
DISCUSSION
Baumann and Metzger (13) suggested that the thyroid has an affinity not only for iodine, but also for other members of the seventh periodic group of elements. Several studies utilizing fluorine (14), chlorine (15), bromine (16), astatine (17, 18), manganese (19), technetium (20) and rhenium (21) have consistently demonstrated the ability of the thyroid to concentrate these elements in a ratio of greater magnitude than that measured in other tissues of the body. However recent experiments using radiofluorine in rats (22) have not corroborated the earlier chemical findings of Chang et al. (14). In our studies with radioactive fluorine, no appreciable uptake of F18 by the thyroid could be detected either in the normal or in the hyperactive gland. The significance of this statement is limited to the accuracy of the measurement, since 1% h-1 of the injected fluorine amounts to 200 jug. per hour, a considerable quantity when compared to the 2-10 ug. of iodine hourly taken up by the thyroid. The results of these studies must therefore be confirmed by studies using carrier-free radiofluorine.
Apart from the possibility of direct uptake of fluorine by the thyroid, another interesting hypothesis is that fluorine could have a mass-action effect on the uptake of iodine. Experiments with simultaneous intraperitoneal injections of radioiodine and fluorine in rats showed no significant difference in the uptake gradient during the first ten minutes (23). Similarly, in our studies, the sharp rise of the plasma fluorine level did not impair the thyroidal uptake of iodine. Under normal conditions the plasma fluorine level is about four times higher than the iodine level and therefore the action of fluorine upon thyroid physiology is not likely to be the result of simple competition between the halogens for receptor sites within the gland.
Although no toxic action of low fluorine intake upon renal function has been reported (24, 25), it could be assumed that an increase in the urinary excretion rate of iodine would cause a secondary reduction of thyroidal uptake. In 2 cases we measured the initial urinary excretion rate of iodine before and after administration of NaF. In 4 cases the urinary excretion rate was calculated from the values of To' and maximum thyroidal uptake (10). No consistent deviation was found.
Another tentative explanation of the depression of the thyroidal iodine-concentrating mechanism is primary inhibition of the synthesis of thyroid hormone, together with a secondary fall of the uptake of inorganic iodine. Thyroidal uptake studies prolonged for seven to ten days, and repeated direct measurements of the level of plasma protein-bound radioiodine before and after fluorine therapy, yield no evidence of such a mechanism.
The only evidence concerning the mode of action of fluorine upon thyroidal function relates to the direct reduction of the uptake rate of inorganic iodine. This interpretation receives further support from 1) the appearance of a goiter, 2) clinical improvement after fluoride therapy, and 3) recurrence of hyperthyroidism when iodine intake was simultaneously increased. Apparently, the inhibition of the iodine-concentrating mechanism is not complete enough in all patients to induce a sufficient degree of iodine deficiency within the gland. Godley and Stanbury (26) observed that when patients were prepared for operation with perchlorate there was a tendency toward relapse when iodine was added during the final stages in order to reduce the vascularity of the goiter. Fletcher et al. (27) described an inhibitory action of perchlorate, thioc yanate, iodide and nitrate upon the I131 concentration in slices of the salivary gland of the mouse. They found later (personal communication) that the fluoride ion at a concentration of 10-3 M depresses the iodide accumulation to about 70-80 per cent of the control value without concomitant depression of the oxygen consumption of the cells. With higher concentrations of fluoride, both oxygen consumption and iodide uptake are depressed. It is therefore not surprising that the action of fluorine upon the thyroidal uptake of iodide in man has been found weak, inconstant and delayed and that hyperthyroidism recurs when blood iodide levels are sufficiently high to raise the concentration within the gland to the level previously reached by the gland's iodide-concentrating mechanism alone.
The main objective of the present study was not to determine whether fluoride is effective, safe and suitable for routine use in the medical treatment of hyperthyroidism. For instance, with the same biologic mechanism of action, perchlorate is a more active drug and its use does not raise the question of possible accumulation in the body. Our aim was to elucidate the inhibitory effect of chronic administration of fluoride upon thyroid function in cases of hyperthyroidism. It was demonstrated that such an action appears only occasionally among persons subjected to massive doses of this substance.
Acknowledgment
The authors are indebted to Miss M. Miller for her collaboration in the tracer studies.
REFERENCES
1. GALLETTI, P.; HELD, H. R.; KORRODI, H., and WEGMANN, T.: Etude experimentale de l'antagonisme iode-fluor chez l'homme, Rev. Suisse Odont. 65: 753, 1955.
2. KORRODI, H.; WEGMANN, T.; GALLETTI, P., and HELD, H. R.: Sind bei der Caries-prophylaxe mit Fluor Ruekwirkungen auf die Schilddruse zu erwarten? Schweiz. med. Wchnschr. 85: 1016, 1955.
3. DEMOLE, V., and LERCH, P.: Normalite du depot d'iode 131 dans la thyroide du rat an cours de la fluorose experimentale, Helvet. physiol. pharm. acta 14: C62, 1956.
4. LEVI, J. E., and SILVERSTEIN, H. E.: Lack of effect of fluorine ingestion on uptake of iodine 131 by the thyroid gland, J. Lab. & Clin. Med. 45: 348, 1955.
5. GALLETTI, P.; JOYET, G., and JALLUT, 0.: Effets du fluorure de sodium sur la fonction thyroidienne dans la maladie de Basedow, Helvet. med. acta 24: 209, 1957.
6. GOLDEMBERG, L.: Action physiologiques des fluorines, Compt. rend. Soc. de biol. (Paris) 95: 1169, 1926.
7. GOLDEMBERG, L.: Traitement de la maladie de Basedow et de l'hyperthyroidisme par le fluor, Presse med. 38: 1751, 1930.
8. GORLITZER, V.: Ein neuer Weg zur Behandlung der Thyreotoxikose mit Fluorwasserstoffsaure, Med. Klin. 26: 717, 1932.
9. GREFNWOOD, D. H.: Fluoride intoxication, Physiol. Rev. 20: 582, 1940.
10. JOYET, G., and GAUTIER, R.: Dynamic theory of the radioiodine investigation of thyroid function, Bull. Acad. Suisse Sc. Med. 11: 82, 1955.
11. JOYET, G.; KOLLER, F., and MORANDi, L.: The initial tangent of the uptake curve as a test for diagnosis of the thyroid function with radioiodine, Bull. Acad. Suisse Sc. Med. 12: 273, 1956.
12. JOYET, G.: Determination du taux de fixation initial du radio-iode a l'aide de deux compteurs a scintillations, Ztschr. f. Isotopenforsch. 1: 11, 1956.
13. BAUMANN, E. J., and METZGER, N.: Behavior of the thyroid towards elements of the seventh periodic group. I. Halogens and thiocyanates, Proc. Soc. Exper. Biol. & Med. 70: 536, 1949.
14. CHANG, C. Y.; PHILIPPS, P. H.; HART, E. B., and BONSTEDT, G.: The effect of feeding row rock phosphate on the fluorine content of the organs and tissues of dairy cows, J. Dairy Sc. 17: 695, 1934.
15. REMINGTON, R.: Effect of chloride on the thyroid gland, Proc. Soc. Exper. Biol. & Med. 37: 652, 1938.
16. PERLMAN, L.; MORTON, M. E., and CHAIKOFF, I. L.: The selective uptake of bromine by the thyroid gland with radioactive bromine as indicator, Am. J. Physiol. 134: 107, 1941.
17. SHELLABARGER, C. J., and GODWIN, J. T.: Studies of the thyroidal uptake of astatine in the rat, J. Clin. Endocrinol. & Metab. 14: 1149, 1954.
18. HAMILTON, J. G.; DURBIN, P. W., and PARROTT, M.: The accumulation and destructive action of astatine211 (eka-iodine) in the thyroid gland of rats and monkeys, J. Clin. Endocrinol. & Metab. 14: 1161, 1954.
19. RAY, T. W., and DEYSACH, L. J.: Storage of manganese by the thyroid, Proc. Soc. Exper. Biol. & Med. 51: 228, 1942.
20. BAUMANN, E. J.; SEARLE, N. L.; YALOW, A.; SEIGEL, E., and LEIDLIN, S. M.: Behavior of the thyroid towards elements of the seventh periodic group. III. Technetium, Fed. Proc. 11: 184, 1952.
21. BAUMANN, E. J.; ZIZMOR, N.; OSHRY, E., and LEIDLIN, S. M.: Behavior of the thyroid towards elements of the seventh periodic group. II. Rhenium, Proc. Soc. Exper. Biol. & Med. 72: 502, 1940.
22. WALLACE, P. C.: The metabolism of F18 in normal and chronically fluorosed rats. Publ. Univ. Calif. Radiation Lab. (Berkeley), No. 2190, 1953.
23. HARRIS, N.O., and HAYES, R. L.: A tracer study of the effect of acute and chronic exposure to sodium fluoride on the thyroid iodine metabolism of rats, J. Dent. Res. 34: 470, 1955.
24. BOND, A. M., and MURRAY, M. M.: Kidney function and structure in chronic fluorosis, Brit. J. Exper. Path. 33: 168, 1952.
25. SCHLESINGER, F. R.; OVERTON, D. E., and CHAIN, H. C.: Study of children drinking fluoridated and non fluoridated water,. J.A.M.A. 160: 21, 1956.
26. GODLEY, A. F., and STANBURY, J. B.: Preliminary experience in the treatment of hyperthyroidism with potassium perchlorate, J. Clin. Endocrinol. & Metab. 14: 70, 1954.
27. FLETCHER, K.; HONOUR, A. J., and ROWLANDS, E. N.: Studies on the concentration of radioiodide and thiocyanate by slices of the salivary gland, Biochem. J. 63: 194, 1956.
Return to Fluoride Bibliography